

Canadaland in Bad Decline, Part Two
Canadaland in Bad Decline, Part Two
The long, slow slide in infrastructure and healthcare


Canada has become a more difficult and less rewarding country to work in of late, but the faltering economy does not suffice to explain the present national malaise or growing political discontent. Our problems are far more grave and far less amenable to democratic retooling than we would like to imagine. Rather, core aspects of the Canadian post-war compact have been badly undermined or eroded, resulting in a declining quality of life and a deepening pessimism about the future.
To understand this shifting mood, you need to grasp something fundamental about the Canadian identity in the late 20th and early 21st centuries. Contrasting itself with its neighbour to the south, which chased excess and influence and above all wealth, Canada sought a middle way. Higher taxes, guaranteed healthcare and generous social protections made Canada a difficult country to become wealthy in (our most ambitious often fled south) but an easy country to live comfortably in. If our highs were not as high, neither were our lows as low, and for decades that equilibrium was a source of national pride.
Today, that vision of Canada no longer pertains. The wealth gap between rich and poor Canadian households grew at the fastest rate ever recorded last year, while housing affordability plummeted in all ten of Canada’s major cities, and key public services, especially healthcare, were stretched to the breaking point, resulting in longer wait times and growing patient dissatisfaction. Unsurprisingly, the confluence of these factors is taking a toll on the subjective well-being of Canadians. According to polling conducted in December of last year, just 31% of Canadians are optimistic about the future of Canada’s middle class, the nadir since this poll’s inception, while just 52% believe their children “can be middle class or higher through hard work,” down from 79% in 2020.
A key plank of this pessimism comes from the country’s declining physical infrastructure and fraying public services, both of which were formerly sources of pride. Consider the Canadian Infrastructure Report Card, issued by a collection of engineers, public works groups, transit associations and municipalities, with the aim of producing a comprehensive assessment of Canada’s physical infrastructure. Their last report, issued in 2019, described Canada’s infrastructure as “at risk,” with these key findings:
Nearly 40 percent of roads and bridges are in fair, poor or very poor condition, with roughly 80 percent being more than 20 years old.
Between 30 and 35 percent of recreational and cultural facilities are in fair, poor or very poor condition. In some categories (such as pools, libraries and community centres), more than 60 percent are at least 20 years old.
30 percent of water infrastructure (such as watermains and sewers) are in fair, poor or very poor condition.
This mirrors our decline in the World Economic Forum’s ranking of trade infrastructure (think roads, railways and ports), from a top-10 placing in the 2000s to 32nd globally and last in the G7.
The average Canadian may be unaware of our declining trade infrastructure, but they experience the sorry state of our roads on a daily basis. The WEF ranks Canada 31st in the world for road quality, below Brunei and Egypt and barely ahead of Turkey, while the CBC estimates that Canadians spend over three billion dollars a year repairing damage caused by potholes. To be sure, some regions are worse than others: CTV estimates that half of Quebec’s roads are in “poor” condition, while GPS company TomTom, in its annual ranking of world traffic conditions, found Toronto to be the third-worst city in the world and worst city in North America for traffic speed, with an average 10-kilometre trip taking nearly 30 minutes of driving time.
More damaging to our national self-esteem than infrastructure and more demeaning to Canadian morale than traffic is the steep decline in the quality of and access to healthcare. Healthcare has been a Canadian priority since the federal government passed the Medical Care Act of 1966, with annual costs now in excess of $340 billion, or nearly $9,000 per Canadian, but the cost of care has long ceased to be commensurate with its quality. Across the country, emergency rooms are at or over capacity, with wait times surpassing 20 hours in the worst areas, resulting in nightmarish newspaper headlines (“BC Woman Dies After 14-Hour Hospital Wait” / “Four in Ten Child Patients Face Unsafe Spinal Surgery Wait Times” / “Teen Waits 19 Hours for Emergency Appendectomy” / “Two Patients Die in ER Waiting Room”) that put a human face on our failures. In the words of Dr. Trevor Jain, a member of the Canadian Association of Emergency Physicians, to Global News: “The situations from coast to coast, they’re horrific and inhumane.”
It isn’t just emergency visits that are cause for concern, however. Canadian hospitals have been accustomed to operating over capacity since long before the COVID-19 pandemic (I have personally witnessed the indignity and discomfort visited on friends and family forced to sleep on a gurney in a hospital corridor rather than on a bed in a closed room), while family doctors and nurse practitioners, the go-to solution for Canadians with non-emergency medical issues, are in short supply, with an estimated 6.5 million Canadians presently without access. Small wonder, then, that The Commonwealth Fund, in its ranking of healthcare access among high-income countries, ranked Canada tenth out of eleven countries, ahead of only the United States, the sole country on the list without a system of universal healthcare.
And what of specialty care? In research conducted by the Fraser Institute and reported on in a document aptly titled “Waiting Your Turn,” the long, slow decline in Canadian healthcare access is made painfully clear:
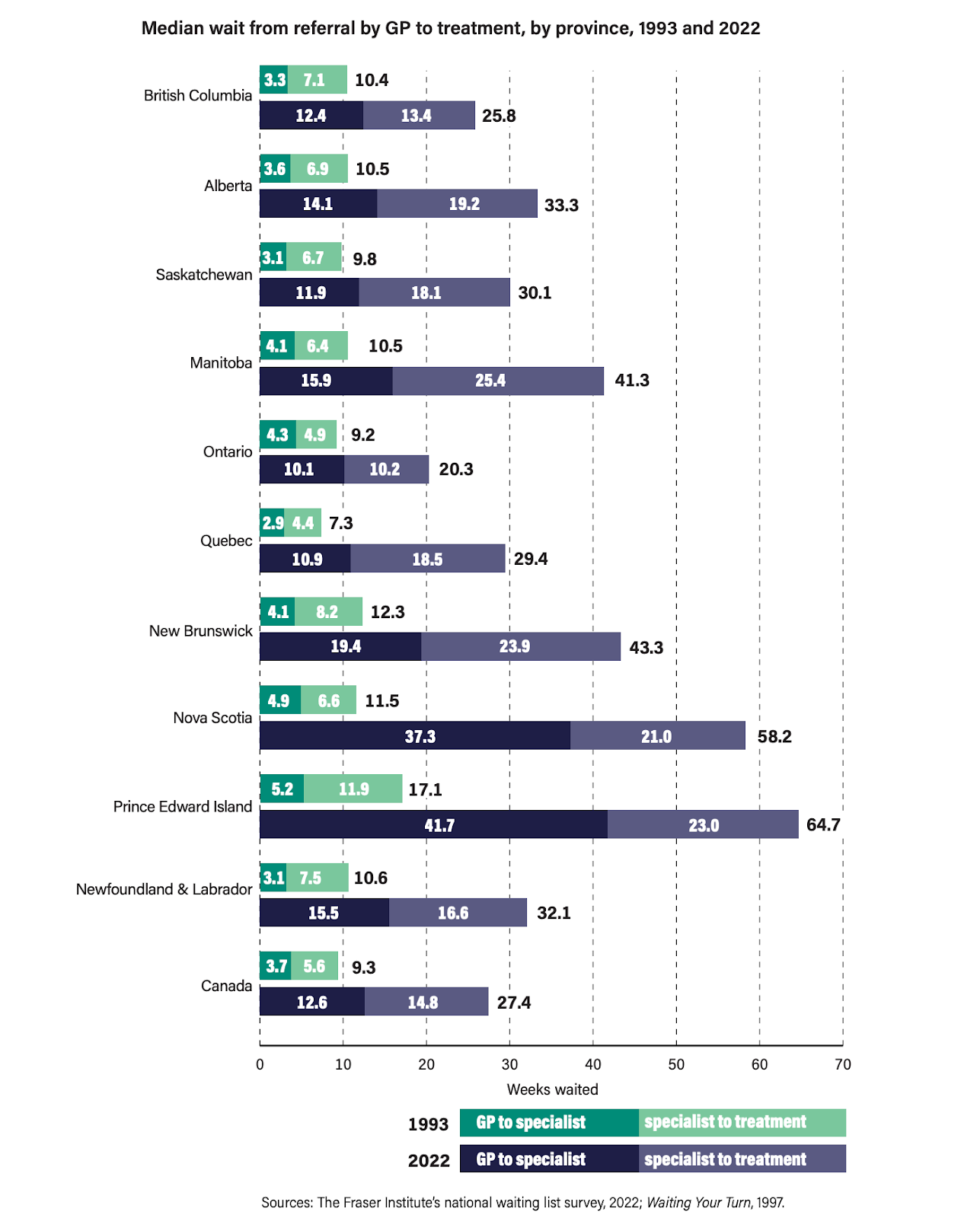
In 1993, across the country, the total wait time from GP visit to treatment averaged just 9.3 weeks, while in 2022, when the report was concluded, that same turnaround time had ballooned to 27.4 weeks, an increase of 195%. Their findings track with an earlier 2016 report, conducted by the Commonwealth Fund, comparing specialist wait times across 11 OECD countries, where Canada ranked dead last for access to specialist care. There are some obvious drivers behind these delays, from the lacklustre expansion of our medical residencies (just 167 new positions added in the last decade) and the massive boom in Canada’s population in recent years to the bloat in hospital administration positions, but the result, for Canadians, has been a catastrophic decline in the standard of care and a serious breach of a fundamental tenet of the Canadian social compact.
For decades, rich and poor alike sought care in the same hospitals under the same basic conditions, with the reasonable expectation of timely and adequate treatment. Today, wealthy Canadians increasingly opt out of the Canadian public system, paying out of pocket for private treatment, while middle class Canadians, far less equipped to discharge the additional expense of private care, must choose between painful and possibly life-threatening delays or taking on medical debt. One story from Maclean’s (“Canada’s health system gave me a choice: years of disability, or $22k for private surgery”) exemplifies the plight of a growing number of Canadians who are not severely ill enough (or old enough) to command priority treatment but nonetheless experience healthcare delays as increases in chronic pain, deteriorating health, and declining quality of life. The latest figures provided by the Canadian Institute for Health Information for three benchmark surgeries (knee replacement, hip replacement and cataract surgery) show that more than 30% of operations are performed outside the six-month wait time, which itself already represents a lengthy delay on the turnaround times possible by paying out of pocket for private treatment.
Once a source of pride and still a major expense, healthcare in Canada is now at a breaking point, and the inadequacy of this most fundamental service is a major driver of Canadian pessimism in a country with a rapidly ageing population. Unfortunately, the story does not end here. Though Canada has gotten noticeably worse at saving and extending lives, it is proving remarkably adept at ending them. In 2015, Canada’s Supreme Court overturned key prohibitions against euthanasia, paving the way for the creation of MAiD (medical assistance in dying) laws, allowing eligible Canadians to receive a merciful death at the hands of the state. Since the program’s inception in 2016 until the end of 2022, the last time figures have been made available, 44,958 Canadians have chosen a MAiD death, with the program’s popularity growing at an annual average rate of 31%.
The controversy, the entire ethical dilemma laid bare by these laws, should be obvious: what exactly makes one eligible for a “merciful death”? In 2016, when the laws were first overturned, the standard offered by the courts was a prognosis of “reasonably foreseeable death” from a “grievous and irremediable” condition, although even this standard was not substantiated by objective medical criteria but left to the judgement of the patient’s own doctors. Since March of 2021, however, even these meagre standards have been dispensed with, after successful challenges from civil liberties groups arguing that long-term disabilities ought not to be disqualified, and, as I write, Canada is actively contemplating expanding the criteria to include mental illnesses (an amendment for which the Canadian Bar Association has expressed support).
The combination of a failing healthcare system, chronically overstretched public services, and expansive right-to-die legislation has already created nightmares. Consider the case of Christine Gauthier, a veteran and former Paralympian who was offered MAiD “services” after five years of unsuccessfully petitioning to have a wheelchair ramp installed in her home. "It was just getting too much and unbearable. And the person at VAC mentioned at that point, 'Well, you know that we can assist you with assisted dying now if you'd like.' And I was just shocked because I was like, 'Are you serious?' Like that easy, you're going to be helping me to die but you won't help me to live?" After her story went public and caused a scandal, four other veterans came forward to confirm they were offered similar “help” by their government.
In another high-profile case, a 51-year-old Ontario woman, identified only as Sophia, was granted MAiD acceptance with the diagnosis of “multiple chemical sensitivities” (MCS), a form of environmental allergy that can be alleviated by, of course, a mere change of environment. According to CTV reporting, “she died after a frantic effort by friends, supporters and even her doctors to get her safe and affordable housing in Toronto. She also left behind letters showing a desperate two-year search for help, in which she begs local, provincial and federal officials for assistance in finding a home away from the smoke and chemicals wafting through her apartment.” In a video recorded eight days before her death, Sophia was blunt: “The government sees me as expendable trash, a complainer, useless and a pain in the ass.”
Sophia’s case highlights the glaring conflict of interest behind the state adopting responsibility over both the life and death of its citizens. Healthcare is expensive, and long-term care even more so. With finite resources, including limited numbers of doctors and hospital beds, might it not be downright selfish to cling to life, especially when a painless death is on offer? Roger Foley, a 42-year-old man left debilitated and bedridden by a neurological disorder, experienced this insinuation first-hand. Disturbed by the coldly utilitarian talk of his healthcare providers, Foley began surreptitiously recording their conversations in his presence. When his requests for at-home care provision were rejected, Foley was instead offered medically assisted death, and in another conversation, a doctor can be heard guessing that Foley’s care costs “north of $1,500 a day.”
Despite repeated assurances by MAiD advocates and Canadian politicians, including Prime Minister Justin Trudeau, that adequate safeguards have been put in place to prevent vulnerable people from opting for an assisted death out of sheer desperation, the on-the-ground realities speak to a darker truth. In a landmark investigate report for The New Atlantis, journalist Alexander Raikin obtained slideshow presentations used in training seminars for euthanasia assessors and providers in which both “poverty” and “inadequate housing” are identified as primary reasons for a patient to seek an assisted death – and are not deemed disqualifying for MAiD. Raikin cites the parliamentary testimony of Madeline Yi, a psychiatrist involved in those same training seminars, who describes the present safeguards as “impotent” and warns that “the Canadian populace and maybe even the legislators are not aware of who has been qualifying for MAID,” before concluding that “the MAiD system has given enormous latitude to euthanasia providers to make the judgement calls about who should be helped to live and who should be helped to die. The result is a system that is highly efficient at finding reasons patients should qualify, not reasons they shouldn’t.”
In the span of a few short decades, Canada’s healthcare system has become an overcrowded and inefficient embarrassment, widening the rift between wealthy and poor citizens. Worse still, the growing inadequacies in terms of both the timeliness and the quality of medical care we offer serve to make our euthanasia program more and more attractive to Canada’s most vulnerable citizens, an unpardonable perversity for which human rights advocates outside of Canada have expressed greater concern and outrage than our own politicians and pundits.
Grave though these declines in the quality of infrastructure and healthcare may be, they are not what worries me most about the trajectory of our country. Rather, it is the damage done to our national self-image, to our promise to each other as Canadians and the social contract built upon that promise, that ought to cause us greatest concern. Until very recently, the Canadian consensus helped to bring together a culturally and linguistically diverse population scattered across a vast country; today, the failure of that consensus threatens to tear us apart.
I write the chapter in a New York trial judges book on end of life care here. We tiptoe around what you document and your sad story explains why it is a long time off before New York will ever come up with a MAID program. The opposition here is just as you have articulated it with the lopsided calculations - cost of care -v- cost of a terminal cocktail. TX for sending this one around. RJM